BACKGROUND
The following article aims to conceptualize a framework that explicitly addresses birth trauma using feminist trauma theory and somatic trauma theory. Integrating a trauma-informed care (TIC) framework is essential to support the trauma-disrupting model. My intended goal is to expand and introduce my concept of trauma-disrupting care (TDC) to shape the future birth trauma research and to integrate both feminist trauma theory and somatics trauma theory in birth work.
Overall, the leading cause of birth trauma is actions of healthcare provider.2–6 Often, people report a lack of communication and care during their birth and postpartum. A lack of communication makes people feel unheard or uninformed of specific practices and procedures.2–6 The main themes identified in birth trauma research are (1) poor communication, (2) extreme pain, (3) invisibility, and (4) a lack of understanding of what is happening in their bodies and birth.2–5,7–9 This can lead to feelings of harm or fear of death towards self or their baby.10 While emergent or high-risk births are more likely to cause birth trauma, low-risk births still pose a risk for a birthing person.4,7
Structurally embedded oppression, such as sexism, racism, ableism, and queerphobia, contributes to experiences of maltreatment from healthcare providers.11–18 Embedded oppression is often implicit, meaning despite compassion and trauma-informed care, healthcare providers will consciously and unconsciously cause birth trauma as current obstetric systems are built on racist, sexist, ableist, and patriarchal ways of knowledge. Obstetric systems aim to achieve quantifiable outcomes that are often at odds with the actual needs of both clients and providers.
From a historical position, the introduction of medicalization changed the view of birth from a typical physiological process to a process that views the body and birth as a machine that could be fixed and manipulated.11,12 Within this paradigm, black people, Indigenous people, and people of colour (BIPOC) are more likely to experience mistreatment during childbirth because of gendered and racial trauma than white people.13 Further, disabled people express being shamed and guilted for their pregnancies and coerced into pregnancy termination.14,19 Disabled people are more likely to have their pregnancy labelled as high-risk and to experience accessibility issues during birth because of embedded ableism.14,19 Embedded homophobia and transphobia lead to higher rates of birth trauma.16,17 Practices and policies that are not adaptive or inclusive of birthing people’s gender identities, sexual orientations, or family structures contribute to experiences of unsafety.18
There can be both individual and communal impacts of birth trauma. Individuals with birth trauma experience flashbacks, anxiety, depression, and hypervigilancy.20,21 Birth trauma can cause tokophobia (fear of giving birth), poor maternal health outcomes, decreased breastfeeding rate, and poor bonding. It can also lead to post-traumatic stress (PTS) disorder.1,20–22 Furthermore, individual medical trauma can cause intergenerational and intercommunal trauma.23
EXPANDING TRAUMA-INFORMED CARE MODEL
Trauma informed care is a framework that recognizes the widespread experience of trauma and its impacts on patients.24 TIC is intended to raise healthcare provider’s awareness of trauma by effectively shifting the question of “what is wrong with you?” to “what happened to you?”25 The goal of TIC is to avoid traumatization and re-traumatization of patients at both operational and individual levels. This means educating providers and organizations on trauma and its impacts on clients.26 The guiding working principles of TIC include safety, trustworthiness, and transparency; peer support, collaboration, and mutuality; empowerment, voice, and choice; and the recognition of cultural, historical, and gender issues, such as racism and sexism.24,27–29
Improved communication between a healthcare provider and client and respect and compassion are considered the primary tools for preventing birth trauma.2,5,9,30–33 Advocates call for integrating TIC at all levels of perinatal care, hoping to reduce rate of PTS from birth trauma.27,33,34 Recommendations for integrating TIC into obstetrics include active listening, understanding the impacts of trauma, screening for past trauma, informed decision-making, and self-reflection.27,34 Unfortunately, the organizational structure of healthcare and misunderstanding of these principles can impede the universal adoption of these methods.35
The TIC model was developed to care for trauma survivors, rather than as an active model to prevent trauma. To prevent effectively birth trauma as birth takes place, we need to expand trauma-informed care to take an active role in real-time healthcare scenarios, such as giving birth. We need a model that centres embedded structural oppression as the overarching cause of birth trauma and in the absence of being able to prevent trauma, we need a model that recognizes the signs and symptoms of birthing people’s trauma responses during giving birth. This can allow care providers to intervene and disrupt trauma response to reduce postpartum PTS symptoms. Incorporating concepts of both feminist trauma theory and somatics trauma theory can expand the framework of TIC. TDC can provide a framework for addressing birth trauma to prevent or reduce the incidence of birth trauma.
FEMINIST TRAUMA THEORY
Trauma-informed care recognizes systemic oppression, such as gender-based violence, as a source of trauma; it does not centre systemic oppression as the main pre-disposition of birth trauma. This intends that TIC does not go far enough to “call-out” obstetrical violence as the primary cause of birth trauma and healthcare providers as the primary perpetrators. The feminist trauma theory places power and control as a main source of violence and trauma as an expected outcome when birthing people interact with a system and medical processes that are sexist, racist, ableist, and indulge in queerphobia. Therefore, we require a framework that centres structural oppression as the leading cause of birth trauma to address the same effectively.
The feminist trauma theory originated as a response to sexual assault survivors critiquing and politicising gender-based violence.36 Feminist trauma theorists argued that trauma must be supported by political movements that counteract the “silencing and denial” of the hegemonic processes of institutions, including healthcare.36,37 Feminist trauma theorists critiqued the American Psychiatry Association (APA) for sexist diagnosis and argued for the suppression of patriarchal participation in women’s trauma.36 These critiques led to the formation of feminist trauma theory. Feminist trauma theorists argue that “mandated institutions of help, especially arms of the state, must be understood as central players in the traumatizing of people and communities. There is a complex relationship between trauma and systemic oppression.”38(p.1300) This understanding of the feminist trauma theory shifts the burden of trauma away from the birthing person to healthcare institutions.39 A feminist trauma lens views the birthing person as the expert of their lived experience. It positions the oppressed and marginalized as the best source of knowledge. It acknowledges that trauma symptoms, such as hypervigilance and dissociation, are often normal responses to continual threats of violence caused by systemic oppression.40 From this perspective, the feminist trauma theory would suggest that birth trauma is a direct cause of institutional oppression.
SOMATICS TRAUMA THEORY
Neuroscience has increased our understanding of how people respond to trauma experiences. It has also helped trauma survivors and therapists understand how trauma impacts the brain and its future responses.41,42 When exposed to threat, the body responds by fight, flight, freeze, or fawning.41–44 These responses result from the previously experienced trauma or a scenario, such as giving birth.41,42 This area of trauma research argues that talk therapy cannot disrupt trauma responses as the brain cannot process cognitive thought when trauma takes place. Instead, a holistic approach to trauma that utilizes both mind and body approach is more effective.41–44
Haines expands somatic trauma theory to argue that somatics is a holistic methodology focusing on intentional change. It recognizes how the individual and the collective are shaped by psychological, evolutionary, biological and emotional, and social and historical norms that are adaptive to resilient and oppressive forces.38,41 Haines explains that transformation is an embodied experience shaped by our social conditions. The three stages of somatics are (1) somatic awareness, (2) somatic openness, and (3) somatic practices.41
During birth, especially during unexpected emergencies, people’s trauma responses can occur despite the best intentions of care providers. However, applying an understanding of somatics to labour and delivery can help care providers recognize and respond to traumatic responses in real time to disrupt the trauma response and, particularly, integrate both touch and speech to address these responses. While somatics during acutely stressful situations is not discussed in the birth trauma literature, there is growing discussion on reducing stress response among first responders and emergency care providers. Notably, at the beginning of a pandemic, researchers demonstrated that access to adequate personal protective equipment (PPE) reduced trauma responses in healthcare workers.45 Centring the needs of healthcare workers in potentially trauma-causing scenarios reduced trauma responses by restoring a sense of power and safety in perceived vulnerable and dangerous situations. Active listening, autonomy, safety, and control prevent and heal trauma effectively.37 Therefore, applying strategies that recognize trauma symptoms as they occur to return a person to a window of tolerance is a practical and likely effective way of preventing or reducing birth trauma.46 The window of tolerance refers to a state of arousal in which one can tolerate emotional and physical feelings, be present (versus dissociated) and feel safe.46 For someone in labour means the person is able to effectively cope with pain and effectively communicate with healthcare providers.
TRAUMA-DISRUPTING CARE
In order to address birth trauma that occurs during labour and delivery, I created a TDC model. TDC moves beyond TIC towards politicised care and acknowledges historical and systematic oppression. It acknowledges roles of healthcare providers in creating and maintaining trauma and systemic oppression and their responsibility to prevent and reduce real-time trauma during birth. This model explicitly addresses trauma that occurs during labour and delivery.
The working principles of TDC are Critical awareness, Reflexive practice, Embodied consent, Deep listening, and Disrupting trauma (CREDD; Figure 1), which stipulates the healthcare provider to:
-
engage Critical awareness of embedded oppression in routine care;
-
do Reflexive practice before, during, and after each birth;
-
seek Embodied consent;
-
practice Deep listening; and
-
preform Disrupting trauma responses (Table 1)
Figure 1. Trauma-Disrupting Care Process
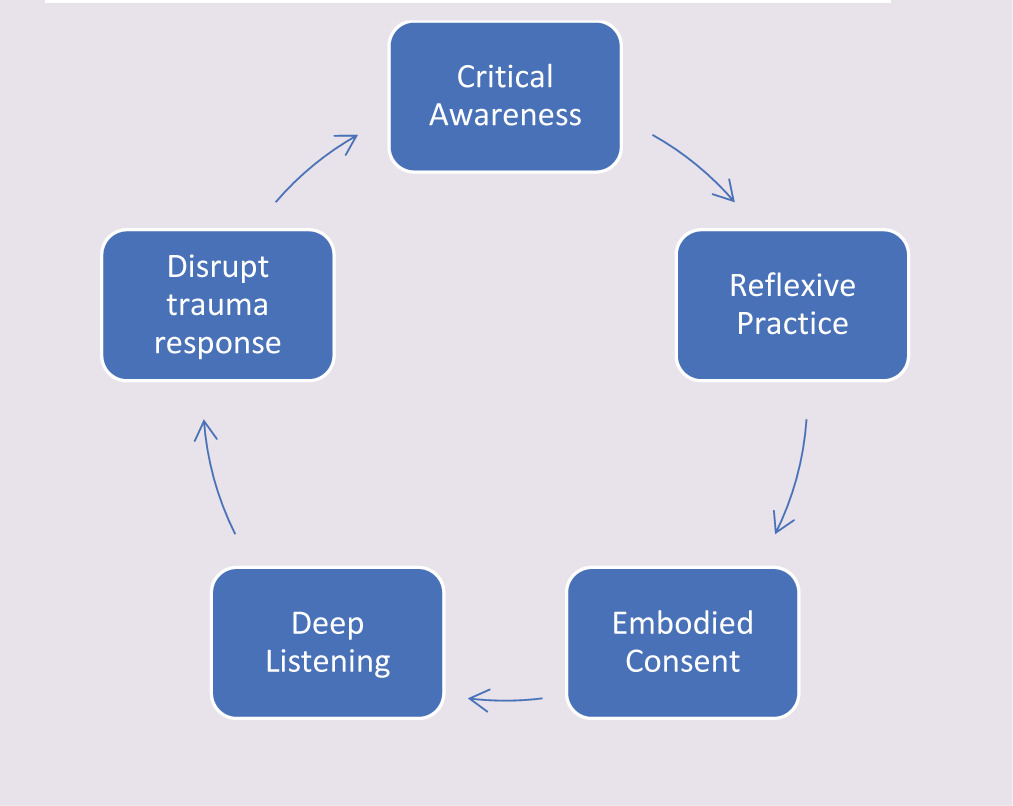
Table 1. CREDD Guide
| CREDD | Guide |
|---|---|
| Critical aware-ness | • Acknowledging your own intersectional identity • Being conscious of power and privilege during birth • Asking: How is my way of knowing impacting the care provided? How are racism, sexism, homophobia, and ableism present in my care and this clinical scenario? • Avoiding fetal-centric care, centering the birthing person first • Recognizing assumptions about the client based on their gender, race, ability, sexual orientation, age, and socio-economic status • Naming systemic oppression and assumptions that are occurring during care to other care providers • Reducing power differentials between client and care provider by seeking embodied consent and deep listening • Validating people’s experience • Understanding how conscious and unconscious biases are present in this client’s diagnosis or clinical scenario • Addressing accessibility needs of the birthing person • Critically examining policies and procedures • Listening, reading, reflecting, and adopting and reflecting |
| Reflexive practice |
Journaling and reflecting 1. What are you practicing? In addition, is what you are practicing aligned with what you care most about? 2. What makes a “good birth”? What makes a “bad birth”? 3. Where did my beliefs on birth come from? How did I learn them? Who did I remember them from? How do I know these beliefs to be true? How do I know these to be untrue? 4. What is an example of a good and bad birth I attended? What was my role? How did the person react? How did I react? 5. What are my thoughts on pain in labour? What are my values and beliefs on pain relief during labour? Critically reflecting, was there a time that someone requested pain relief and I did not meet their request? Why? What does it mean to be too late for an epidural? Do I believe that non-medicated births are superior to medicated births? Do I think that medicated birth is superior to non-medicated births? Why? How has this belief impacted my care? 6. Think about a birth that you thought was “beautiful,” but then the client expressed trauma symptoms from the birth; in detail, what happened? What were your thoughts and feelings during the birth? What do you think the birthing person was experiencing? What did they say during the birth? What did they not say during the birth? Did they have an opportunity to move freely, make choices, and achieve adequate pain relief? Be at their attended choice of birthplace? How were their power and control compromised during the birth? What was your role in creating trauma? How did you debrief with the client? What did you say to the person after the birth? How did you react when the person expressed symptoms of trauma? What could you have done better? How were sexism, racism, ableism, homophobia, and ageism present in their birth? How did you attend to their intersections of identity? On-the-spot reflection using STOP67 (stop, take a breath, observe, proceed) during birth 1. Stop: Take a moment to pause 2. Take a breath: Reconnect to your breath 3. Observe: What is going on in this clinical scenario? How do I know this to be true? What is the client likely feeling? Ask the client, what their feelings are? How am I attending to power dynamics in this clinical scenario? What is their birth plan or intentions? Am I listening to these needs? How can I attend to these needs? What can I do to preserve aspects of their birth plan? What do I think should happen? What is my role? 4. Proceed: Make a conscious decision on how to proceed during care, be transparent, and seek feedback from the client. Communicate with other team members. Be clear with your limits, i.e., are you too tired to continue with care? Debriefing with clients postpartum 1. Personal reflection: What did I think about this birth? Think about how you acted during birth. Was there a better way of doing things? What did you like? What did you do that you did not like? How do you know this to be true? What did you say or not say? Was it helpful? 2. With the client: Would you like to go over your birth? No: Do not review birth but give permission to revisit it anytime. Tell me about your birth. Yes: What are your thoughts, feelings, and sensations about your birth? Do you have any questions? What are the aspects of your birth you thought were good, reassuring, positive, etc.? What are the elements of your birth that you would change? If you feel comfortable, what did you find helpful about our care? What would you have changed? Validate people’s feelings about their births and provide opportunities to review their birth at any point postpartum 3. Seek feedback from clients |
| Embodied consent | • Honesty and transparency: What are you seeing? What do you think might happen? • Taking time to explain the procedure thoroughly. What is it? What can they expect? Why are you doing it? Does the person have any questions? • Letting the birth person choose their support people to be present • Transparency and clarification: Why are you recommending a procedure? • Are you communicating in a way that the birthing person understands? • Reflecting with the client, what is important to them to include in their birth, such as a cesarean section? • Going slow • Being aware of body responses: Pause and check in with the client if the body is tense. Do they want you to continue? Do they want you to stop? • Stopping immediately, if they want you to stop • If their body is pushing you away, stop • Not doing additional procedures they did not consent to, for example, a stretch and sweep, artificial rupture of membranes etc. • Understanding that if someone is in a vulnerable position, such as having a vaginal examination, the procedure should be stopped before offering or recommending something else. • Being aware that consent during duress is difficult • Being aware of power and privilege. How would it look like for someone to consent or not consent? • Reflecting if you are providing an opportunity for them to consent or decline? |
| Deep listening | • Consider doing a body scan when entering a birthing space • Consider doing a body scan throughout the birth • Listening and being aware of sights, smells, and sounds • Allowing space for silence • Querying how do you feel in silence • Slowing down • Reflecting: What do you think this person is feeling, what are their sensations, and what their body language is saying? • Asking: What are you feeling, what are your sensations, what are your thoughts? • Validating emotions during labour, permission to feel whatever they are feeling: “It’s ok to be scared, excited, happy, whatever you are feeling let it be there. You have room in your body for all the emotions.” • Applying therapeutic touch with consent • Checking in with client • Words are powerful! • Before you say something, consider: How is this helpful? Why am I saying this? Is this for me? An example of this is: “It’s ok.” Is it ok? How do you know it is ok? Do you need it to be ok? |
| Disrupt Trauma | • Recognizing signs and symptoms of a fight, flight, freeze, or fawn response • Employing SCOPE Safety Aid with the client: Slow down, Connect to your body, Orient, Pendulate, and Engage (https://traumahealing.org/scope/) • Helping to regulate breathing with the client • Helping orient the client to the surroundings (room) between contractions • Avoiding telling a client that they are “safe” unless these are the words they request you to use, as this could be dysregulating • Using therapeutic touch to help ground a client during birth • Explaining to them why they might be feeling certain ways in their bodies • Helping preserve their birth plan, such as the use of music, skin-to-skin contact • Promoting skin-to-skin unless the client declines • Talking them through the procedure, let them know what sensations they might feel • Providing warmth, such as blankets, heating pads, etc. • Responding to their pain relief requests • Providing eye contact with the client • Avoid using “don’t be scared.” |
1. Critical awareness
The understanding and acknowledgment that racism, colonialization, sexism, ableism, and queerphobia, embedded in healthcare structures and resulting in the continual perpetuation of systemic oppression, are paramount to TDC.38,39 These structures lead to the undermining of birthing people and their communities. By acknowledging that the birthing system is inherently oppressive, care practitioners recognize their roles in maintaining institutional oppression, which contributes to birth trauma, and begin to disrupt birth trauma. It is essential to acknowledge the intersectional identities of care practitioners and clients. In other words, “critical insight that race, class, gender, sexuality, ethnicity, nation, ability, and age operate not as unitary, mutually exclusive entities, but as reciprocally constructing phenomena that shape complex social inequalities.”47(p.3) Developing critical awareness must be a continual reflexive and active practice to name and end systemic oppression in obstetrical care. It begins with understanding the historical and current context of birth and the birthing person to ensure that care practitioners are aware of explicit and implicit bias.
The feminist trauma theory requires us to name oppression, to advocate, and to keep ourselves and our colleagues accountable while recognizing how our intersectional selves and our own identities can make this difficult in the face of hegemonic processes in healthcare.48 Listening, understanding, supporting, and participating in birth movements that aim to decolonize, diversify, and disrupt systemic oppression in birth work is critical. Movements such as returning birth to Indigenous communities, inclusion and promotion of BIPOC midwives and doulas, creation of accessible birthing spaces, gender-affirming language, creating accessible fertility services, and queering birth targets embedded systemic oppression that underpins obstetrics in Canada.16–18,49–53
2. Reflexive practice
Reflexivity is mandatory for ethical and responsible practice. Reflection involves the practitioner examining critical and non-critical incidents to understand their thoughts, feelings, sensations, and assumptions. In contrast, reflexive practice involves becoming critically aware of embedded power structures in care and understanding the incident from multiple perspectives.54–56 It is “recognizing authority over and responsibility for personal and professional identity, values, action, feelings; contestation of lack of diversity, imbalance of power (and) the blocking capability of managerialism… Willingness to stay with uncertainty, unpredictability, doubt (and) questioning.”56
Reflexive practice is part of critical awareness, and it is essential for understanding and preventing birth trauma. It requires practitioners to examine their roles in care and beliefs about what makes a “good birth” and to take responsibility for their actions during perinatal care. Reflexive practice is particularly important to prioritize the psychological well-being of the birthing person over the agenda of a healthcare provider.9 Reflexive practice integrates the feminist trauma theory by recognizing the role of power and structurally embedded oppression in the care of healthcare providers. If birth trauma is caused by the actions and inactions of care providers, reflexive practice can foster the care provider’s understanding of their roles in the creation and prevention of birth trauma. Care providers can do an on-the-spot reaction, and more extended reflection and reflexivity can be done by journaling and debriefing with colleagues, supervisors, and the birthing person themselves.54,56 A healthcare practitioner should do reflexive practice throughout and after each birth.
3. Embodied consent
Informed consent is a practice standard in Canadian healthcare.57,58 Informed consent means patients have been provided with all necessary information, including risks, benefits, alternatives, and recommendations required to consent. Embodied consent expands this understanding and seeks to include information received from the body in the form of sensations, feelings, and intuition.41 It also includes birthing person’s embodied knowledge (knowledge generated through a person’s sensations and ways of knowing) of oneself and their birth.
Seeking embodied consent from our clients is necessary to prevent birth trauma, as it recognizes that people’s words and bodies are not always in agreement.43 This intends that even though a person verbally consents to a vaginal examination (for example), her body that becomes tense and pushes away is saying “no.” It also recognizes that extreme stress, such as emergencies, can make consent difficult. Seeking embodied consent is necessary for client–healthcare provider scenarios because birthing people, especially survivors of trauma, often have learned to override their feelings to appease others.43 The feminist trauma theory would suggest that this is especially true in healthcare relationships that view the healthcare provider (midwife, doctor, nurse, etc.) as expert and the patient as recipient.39 Systemic oppression can lead to silencing of clients, and being aware of this power imbalance urges the care provider to seek embodied consent from clients. Seeking embodied consent requires healthcare providers to be in tune with their own thoughts, feelings, and sensations during birth.
4. Deep listening
Deep listening requires healthcare provider to listen to the inaudible by engaging sound, touch, smell, and taste.59 Engaging in deep listening is engaging in deep self-silence.59 This means being reflexive and present to the birthing person. Deep listening requires critical awareness, reflexive practice, and practicing embodied consent. Acknowledging that the birthing person is the expert of her own body, it is listening to a birthing person with all your senses and ensuring that you are giving adequate time and space for her voices to be heard and respected.
Learned voicelessness is often a consequence of trauma resulting from systemic oppression. Hardy explains that voicelessness denies people their personal power, their agency, and the ability to speak and advocate for oneself.60 Deep listening requires healthcare providers to critically reflect and take responsibility on how their presence, their identities, and their power contributes to the birthing space. Deep listening can disrupt trauma because it requires the healthcare provider to listen holistically and critically to the birthing person, the birthing space, and themselves. Improving communication between birthing people and their care providers is a component of preventing birth trauma.2,5,9,30–33
Engaging in deep listening with the birthing person requires time to orient into the birth work environment. It asks the person what they feel (scared, excited, etc.) and what sensations they feel in their body. It validates these thoughts, feelings, and sensations and normalizes these responses. Observing body movements or immobility can give the practitioner insight into therapeutic touch. Comprehensive deep listening requires time. Deep listening in an emergent scenario is actively slowing down or pausing (even briefly). Deep listening requires the healthcare provider to make an active and political decision to slow down. Slowing down and creating space in healthcare resist healthcare need for speed and efficiency while also allowing for birthing person to be heard.61–63
5. Disrupt trauma responses
Disrupting trauma responses adopts a bodily understanding of how trauma occurs while also utilizing feminist trauma theory that acknowledges that trauma responses are often typical reactions to an atypical (traumatic) scenario. It recognizes the signs and symptoms of trauma (fight, flight, freeze, and fawn) and provides care to re-regulate birthing person. The use of somatics is often applied in trauma therapy. I am proposing applying these techniques during birth (especially in an emergency scenario) and being acutely aware of the signs and symptoms of a trauma response. Simple techniques with consent, such as holding someone’s hand, therapeutic touch, sitting beside them during a complex procedure, helping a client regulate their breathing, providing warm blankets, etc., are compassionate care and may help to re-regulate the client.
While this has not been discussed explicitly in research, a few examples of trauma disruption originate in anesthesia.64 Vogel suggests being psychologically in tune with needs of a client during procedures and responding in an active and in-tune manner.64 Additionally, a small random control trial (RCT) examined the use of skin-to-skin contact to prevent PTS disorder.65 The results demonstrated that immediate skin-to-skin contact for the first hour without disruptions (neonates not being assessed at the warmer) reduced PTS symptoms of people who were identified to have traumatic births.66 While this is a small RCT, it shows promise in integrating somatic principles to reduce birth trauma. While research is needed to explore somatics to prevent PTS from birth, applying somatics may provide active and straightforward methods to reduce or prevent PTS from birth.
SUMMARY
For TDC to be effective, obstetrical care should be client-centred and trauma-informed. TDC requires one-to-one care and should strive for continuity of care as these are important aspects to prevent birth trauma.2–6 Continuity of care helps to build trust between the client and the provider and provides the opportunity for healthcare provider to demonstrate their trustworthiness.
Trauma-disrupting care is an extension of TIC to address trauma as it occurs during birth. The TDC framework theoretically stems from the feminist trauma theory and somatics trauma theory that recognize that the cause of birth trauma is often embedded in systemic oppression and obstetrical violence perpetuated by healthcare institutions and providers and recognizes trauma responses as they occur during birth.
The TDC framework holds potential to prevent birth trauma as it takes place. By recognizing and addressing embedded oppression that is entrenched in birthing care through advocacy and adopting CREDD during labour and delivery, healthcare providers can hopefully address the systems of oppression that cause birth trauma.
LIMITATIONS
As this is a conceptual framework, the future research should investigate whether this model effectively prevents and addresses birth trauma. While this frameworks centres systemic oppression and obstetrical violence as a main cause of birth trauma, an isolated framework cannot adequately address deep embedded colonialization, racism, ableism, queerphobia, and sexism intertwined in healthcare. Healthcare providers must listen and adopt practices advocated by BIPOC, and disabled and queer communities must be integrated into universal practice to address comprehensively systemic oppression in obstetrical care.